Lead Exposure and Oxidative Stress a Systematic Review
![]()
Pb Exposure and Oxidative Stress—A Life Course Approach in U.S. Adults
Department of Built Environment, North Carolina Agricultural and Technical State University, Greensboro, NC 27411, USA
Received: 17 June 2018 / Revised: 25 July 2018 / Accepted: 27 July 2018 / Published: 1 August 2018
Abstruse
Lead exposure and a marker of oxidative stress (gamma-glutamyl transferase—GGT), and their furnishings on life course variables (age, state of nativity, education levels, gender, ethnicity, income, and occupation) were explored in this cantankerous-sectional study of United States (U.South.) adults' ≥ xx years of historic period via the National Health and Nutrition Exam Survey (NHANES) 2007–2010 datasets. State of birth, education levels, gender, ethnicity, income, and occupation showed significant differences depending on the degree of lead exposure, with college levels of exposure resulting in worse outcomes. Age and GGT were significantly associated with lead exposure. More must be washed to mitigate sources of lead exposure, to prevent it from altering the life course of at-gamble populations.
one. Introduction
The life grade theory is one that tin can be used to empathise the factors that touch atomic number 82 exposure risks and disease outcomes. It tin can exist defined in this context equally a study of long-term "biological, behavioral, and psychosocial processes that link adult health and disease risk to physical or social exposures interim during gestation, childhood, adolescence, earlier in adult life or beyond generations" [ane]. The theory states that developmental processes such as delayed evolution or environmental atmospheric condition in utero, which are averse to proper growth and development, are associated with an increased risk of centre and afterward life illnesses [1,2].
In the model, there is a belief that many of the chronic and adverse wellness outcomes are created early in development in utero and then bring forth lasting damage to the adult after on. The theory too speaks of damaging physical and social environments which create pathology and induce toxic changes in the body that affects the private from in utero through machismo due to cumulative exposure [iii]. Modification of the adverse experience is key in mitigating the effects of the exposure [ane].
Time and place are primal components of the life grade framework. Time refers to non only lifetime (i.e., chronological age) merely besides historical time (i.east., a birth cohort). The birth cohort is the year of nascency during which important environmental weather occur that can affect the health of children in the present and could manifest at a later on phase of life [one].
Identify is regarding a geographical location and group membership is relating to "family, friends or historic period, and on the basis of class, ethnicity, residence, and gender that arise out of the social and economic structure of society" [4].
The irresolute environment one is exposed to determines and affects their risk of affliction and how they respond to that take a chance [1]. Accumulation of take chances is a concept of the life course approach which posits that insults build upwards due to injury, affliction, environmental atmospheric condition and health behaviors. The life course approach has the objective of testing the extent of cumulative damage to the body as the severity and duration of the exposure increases every bit the body grows older, it is less likely to handle the damage or repair it [4]. Ultimately, the life course approach offers perspective on disease inclinations, and for "gender, ethnic, and geographical, inequalities in health" [4] and is a means to understand lead exposure among U.South. adults.
Lead, a toxic metal, induces numerous agin clinical outcomes in children and adults. Due to the widely held view that pb had the capacity to enhance engine performance by boosting octane ratings, reduce engine knocking, and optimize the performance of valve seats within motors, United States motor vehicles used gasoline containing tetraethyl lead additives from the 1920s to 1995 [five]. Information technology plays no role in normal human physiology and through diverse mechanisms, about involving taking calcium's identify in mechanisms of physiological importance, acts to induce agin clinical outcomes [vi,7]. Additionally, because atomic number 82 persists in the environment, populations can remain exposed in areas where it was used previously. Lead exposure has decreased significantly over the by 30 years in the U.Southward. because of policy-driven changes which has acquired atomic number 82 content to be reduced in gasoline, household paint, the nutrient canning process, industrial emissions, and in water [eight]. However, despite the dramatic fall in pb exposure in the U.S., certain segments of the population go along to exist exposed to elevated levels of lead due to their socioeconomic status, occupation, their place of residence (especially, living in disadvantaged neighborhoods), and/or their history of exposure [8].
Oxidative stress, a process which produces reactive oxygen species (ROS) or reactive nitrogen species (RNS), is an imbalance between the pro-oxidants and antioxidants in the body [9]. Pro-oxidants may exist either exogenous or endogenous. The harmful effects of free ROS and RNS are potential biological damage where at that place is either a asymmetric production of ROS/RNS and/or a deficiency of antioxidants. The redox stress/oxidative stress is a complex process which impacts humans depending on the type of oxidant, on the limerick and activities of various antioxidants on the site and intensity of action, and on the ability of repair systems [9].
Under normal conditions, the physiologically of import intracellular levels of reactive oxygen species (ROS) are maintained at depression levels by diverse enzyme systems participating in the in vivo redox homeostasis.
Oxidative stress affects the vascular system, a organization of import to normal physiological role. With respect to vascular oxidative stress, reactive oxygen species (ROS) including such enzymatic processes as xanthine oxidase, Nicotinamide adenine dinucleotide phosphate (NADPH) oxidase, and an uncoupled endothelial nitric oxide (eNOS) synthase, that possibly affects vascular tone or office, past altering information technology through its effects on nitric oxide (NO) signaling or bioavailability [10]. NO that is released from endothelial cells works in concert with prostacyclin to inhibit platelet assemblage. Specifically, the NO inhibits the attachment of neutrophils to endothelial cells and the expression of adhesion molecules. In elevated concentrations, NO inhibits the multiplying of smooth muscle cells; thus whenever NO arrears is encountered, atherosclerosis may exist initiated or potentially accelerated [10]. With respect to the connection betwixt antioxidant nutrients and lead exposure, Hsu and LeonGuo [11] institute that lead-induced oxidative stress plays a function in the pathogenesis of lead poisoning by affecting the delicate antioxidant/pro-oxidant equilibrium in cells. They establish that in vivo studies advise lead exposure induces the generation of ROS and amending of antioxidant defense systems in occupationally exposed workers. Various markers exist for oxidative stress including erythrocytes glutathione (GSH) levels, plasma malondialdehyde (MDA), nitrite/nitrate (NOx) and homocysteine (Hcy) levels, besides as serum ceruloplasmin (Cp), total antioxidants (TAO), endothelin-1 (ET-1) levels and γ-glutamyl transferase (GGT) [12]. In this study, GGT levels volition exist used as the marker of oxidative stress. Epidemiological studies have consistently suggested that serum GGT within its normal range might be an early and sensitive enzyme related to oxidative stress [13,fourteen].
Operationalization of Theory
The life class theoretical model will be operationalized in this study as shown in Figure 1 using variables and conditions widely reported in the literature [xv,16,17,18].
In the diagram, path A represents a biological pathway where the lead exposure is associated with agin wellness outcomes in childhood and adulthood. It should exist noted that atomic number 82 has a half-life of up to 30 years in bone; thus, exposure in utero can continue to accrue and induce health effects over one's lifespan. Path B is a social pathway where i's socioeconomic background increases their run a risk of exposure to lead which can subsequently accumulate over a lifetime and in the presence of new and acute exposures induce agin health effects. Path C is the sociobiological path that indicates the social and economic status of an individual and how continuous exposure can increase over a lifetime and later on induces affliction. Path D represents a biosocial pathway in which the consequences of all-encompassing lead exposure results in decreased educational attainment and subsequently brings virtually poverty. Ultimately, what this model shows is that exposure during a key flow may event in the irreversible induction of pathology [19] which affects an private through their lifetime. Regarding lead, when it damages some biological functions, especially in the neurological system, the damage may exist irreversible making prevention vital.
Prevention starts early, during in utero as toxicity associated with lead crosses the placental barrier and the fact that it competes with calcium, thus affecting fetal and maternal bone function [xx]. Maternal os is an endogenous source of pb; since a woman who has accumulated lead during her lifetime and in her reproductive years, may take a significant store of atomic number 82 in her bones. This accumulation suggests that women who have been exposed to atomic number 82 in the past are at risk of exposing the developing fetus to pb via cord blood and later on nativity, through chest milk [21]. Lead exposure can then kickoff to build upwards through babyhood and into adulthood.
Developed Blood Lead Epidemiology Surveillance (ABLES), which monitors adult blood lead levels (BLL) in the United States [22], adopted v μg/dL as the reference for elevated BLLs in adults. Lead exposure among adults mainly occurs in the workplace within lead and zinc ore mining, painting, and battery manufacturing industries. Exposure in these and other industries can occur over the course of one's life and through mechanisms including oxidative stress and induce pathology. The electric current study examined atomic number 82 exposure and sought to determine if it alters key life course variables in a nationally representative sample. It likewise sought to understand the role of oxidative stress; one of the underlying mechanisms for much of the pathology, due to lead exposure.
2. Materials and Methods
Information from NHANES 2007–2010 were used to study lead and oxidative stress biomarker GGT in the general U.S. adult population. The NHANES 2007–2010 survey, conducted by the Centers for Disease Control and Prevention (CDC), used a representative sample of the U.S. noninstitutionalized civilian population. Participants were selected using a complex sampling methodology. The sample weights for NHANES 2007–2010 were based on population estimates that incorporate the national demography count. In all, 12,153 adult subjects ≥ 20 years were involved in this complex, multistage, stratified cluster survey in 2007–2010, which after because sampling weights consisted of 217,057,187 people. Of the 12,153 participants, BLL was measured in 9781 adult subjects which represented an estimated 182,052,299 people.
NHANES 2007–2010 consisted of a standardized questionnaire and a physical exam at a Mobile Examination Center (MEC). The data is bachelor at the arrangement'due south homepage. Methods for data collection are on the NCHS' website [National Center for Health Statistics, 2007–2008, 2009–2010].
2.1. Biomarkers in the Operationalized Theoretical Model
The biomarker of interest is blood lead, which is representative of current lead exposure [23]. Blood lead level (BLL) can help determine the level of exposure but is not representative of the body burden of lead. Other biomarkers include GGT, which tin be used as a measure of oxidative stress. In NHANES 2007–2010, the biochemistry biomarkers were measured via the Roche Modular P chemical science analyzer at the University of Minnesota, MN, USA and a Beckman Synchron LX20, Beckman UniCel® DxC800 Synchron (Brea, CA, USA) at Collaborative Laboratory Services. Metal assays in whole blood samples were performed in the NHANES 2007–2010 at the Partitioning of Laboratory Sciences, National Center for Environmental Health (NCEH) of the CDC.
2.2. Statistical Analysis
In this study, the analysis was performed on those experiencing various degrees of exposure represented past BLLs in three tertiles; 0–2 µg/dL, 2–5 µg/dL, 5–ten µg/dL, presented equally tertile 1, tertile 2, and tertile iii in this study.
The clan betwixt lead and the oxidative stress marker were examined with linear regression. Natural log transformation was used for contained and dependent variables in regression analysis as the variables of involvement were non unremarkably distributed.
Data analysis and management was done in accordance with the NHANES analytical guidelines relating to its survey design and weighting. The software Stata SE/15.0 (StataCorp, College Station, TX, USA) was used.
A p-value of <0.05 was considered significant while a value of <0.10 was considered moderately meaning.
three. Results
3.1. Country of Nascency
Results for the country of birth over the tertiles of exposure are shown in Table 1. Those born in Mexico were disproportionately represented among those in the higher tertiles of exposure.
3.ii. Education Level
The educational level categories of the surveyed participants included those who attained less than Grade 9, those with 9th to 11th Class educational level (including twelfth grade), those with a High Schoolhouse diploma, those with some College or Acquaintance Degree (AA), and those who completed Higher. The complete results of the surveyed participants' educational attainment are displayed in Table ii below.
three.iii. Gender
The results of the different gender categories and tertiles of exposure are shown (in percentages) in Tabular array 3 below.
iii.4. Ethnicity
The ethnic groups constitute in the data included Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black, and Other Race which included multi-racial. The results are shown (in percentages) in Table 4 below.
3.5. Income
Income and its role in atomic number 82 exposure is demonstrated in Tabular array 5. Trends evidence that those of lower incomes were represented in higher proportions in the lowest income groups.
three.6. Occupation
Occupation and its manifestation in the teritles of exposure are shown in Table half-dozen. Note that agriculture, forestry and line-fishing, along with construction had a higher representation in the highest tertiles of exposure.
3.7. Historic period and Oxidative Stress
Historic period and oxidative stress biomarker GGT and their relation with BLL over the tertiles of exposure are presented in Table seven beneath.
The associations of BLL, presented as the natural log of BLL (lnBPb) with age and GGT are presented in Table 8 below.
4. Discussion
4.i. Atomic number 82 Oxidative Stress and the Life Grade
Lead exposure tin can be understood through a life course approach. Exposure can brainstorm in utero with hazard continuing into adulthood. The xxx-yr one-half-life of pb in bone, an endogenous source of lead exposure, is such that exposed populations remain exposed during their lifetime. The current study, one of the first to examine lead exposure, oxidative stress, and life form variables in a nationally representative sample had several key findings. Regarding country of nascence, those born in United mexican states had significantly college pb exposure than those built-in in the U.S. One may refer to the sociobiological pathway where existence born in Mexico, which has non enjoyed the regulatory successes [24] of the U.Due south., may get out some populations exposed to excess levels of atomic number 82. In improver, Mexican-Americans and Non-Hispanic Blacks were represented in higher proportions in the college exposure tertiles than others. Those with amend education also had less lead exposure. The work of Bellinger and colleagues [25] which found that slightly elevated blood atomic number 82 levels around the age of 24-months were associated with intellectual and academic operation deficits at age x-years. In this report, those of lower income were represented in more than in the highest tertile of exposure. One may refer to the biosocial pathway of the life course approach where potentially altered biology lowers ane'southward socioeconomic status. It too speaks to the social pathway where one's socioeconomic status increases their risk of exposure. Agriculture, forestry and fishing along with construction were more represented in the highest tertile of exposure as compared to other occupations. The structure industry has historically been a source of lead exposure amid adults [26]. Regarding gender, males were more represented in higher tertiles of atomic number 82 exposure than lower tertiles. Accumulation of risk was demonstrated in this report every bit higher doses of exposure resulted in more than adverse outcomes for sociodemographic and clinical indicators.
The current study constitute a statistically significant association between pb exposure and oxidative stress bio-marker GGT. The inquiry of Lee and co-authors backs this as they found associations, in an analysis of NHANES Iii, between blood atomic number 82 and GGT in adults [27]. One of the consequences of lead exposure is oxidative stress. Generation of ROS/RNS via the mitochondrion [28] has potentially severe consequences. The consequences of oxidative stress in the life course is such that information technology can contribute to the pathogenesis of various diseases such equally neurodegenerative diseases [29], cardiovascular diseases [30,31], hepatobiliary diseases [32], and renal disease [33]. The ROS/RNS produced in the tissues can inflict directly damage to macromolecules, such every bit lipids, nucleic acids, and proteins [34] which brings forth much of the pathology associated with oxidative stress.
4.2. Limitations
Measurement of BLLs does non point longer-term exposure; rather, it is indicative of recent lead exposure too as lead that has been mobilized from bone or other tissue sources with no ability to distinguish between both. Measuring of bone lead levels, particularly tibia lead level, via K-Shell 10-Ray Fluorescence (KSXF) would accept provided more information on the length of exposure as bone lead levels are indicative of long-term cumulative exposure to lead. Both the BLLs and os atomic number 82 levels, taken together, would take provided the best and most comprehensive view of the participant's exposure. [35] The electric current cross-sectional report depicts simply a snapshot in time. A longitudinal written report of the grouping may have yielded dissimilar results as people's unique circumstances (finances, family, etc.) change resulting in people moving to unlike parts of the country, creating new social networks, gaining access to necessary cognition about atomic number 82 exposure and hence relocating to safer areas in which exposure is limited.
5. Conclusions
The life class approach may be explained lead exposure during the i'south lifetime. Exposure to lead increases with age; as does oxidative stress. The current study found a pregnant clan betwixt lead exposure and oxidative stress and age. The trajectory of one'southward life may exist significantly altered, starting from where they were born, which may outcome in the exposure to toxicants such as lead which could afterwards touch biological systems, for example, the neurological, cardiovascular, and hepatic arrangement, ultimately altering income, pedagogy levels, and occupation. In U.S. adults, this information suggests that such changes may impact ethnic minorities more then than others. More than must be done to mitigate lead exposure for vulnerable populations in order to promote the human evolution of all in, line with national development goals.
Author Contributions
E.O.-One thousand. wrote the paper and analyzed the data.
Funding
This research was funded from Emmanuel Obeng-Gyasi's research account provided by the United States Department of Education through its Title III initiative.
Acknowledgments
The author would like to acknowledge the National Eye for Health Statistics of the U.Southward. Centers for Disease Control and Prevention (CDC) for its invaluable piece of work conducting the National Wellness and Nutrition Examination Survey.
Conflicts of Interest
The author declares no conflict of interest.
References
- Kuh, D.; Shlomo, Y.B. A Life Course Approach to Chronic Disease Epidemiology; Oxford Academy Printing: Oxford, UK, 2004; Volume 2, p. three. [Google Scholar]
- Pollitt, R.A.; Rose, Yard.M.; Kaufman, J.S. Evaluating the Prove for Models of Life Course Socioeconomic Factors and Cardiovascular Outcomes: A Systematic Review; BMC Public Wellness: London, U.k., 2005; Volume v, p. i. [Google Scholar]
- Barker, D.J. Fetal and Babe Origins of Adult Disease [Monatsschrift Kinderheilkunde]; Spinger: Berlin, Germany, 2001; Volume 149, pp. S2–S6. [Google Scholar]
- Kuh, D.; Ben-Shlomo, Y.; Lynch, J.; Hallqvist, J.; Power, C. Life Course Epidemiology. J. Epidemiol. Customs Wellness 2003, 57, 778–783. [Google Scholar] [CrossRef]
- Mielke, H.W.; Laidlaw, G.A.; Gonzales, C. Lead (Lead) Legacy from Vehicle Traffic in Viii California Urbanized Areas: Continuing Influence of Pb Dust on Children'due south Health. Sci. Total Environ. 2010, 408, 3965–3975. [Google Scholar] [CrossRef] [PubMed]
- Pounds, J. Effect of Lead Intoxication on Calcium Homeostasis and Calcium-Mediated Cell Function: A Review. Neurotoxicology 1984, v, 295–331. [Google Scholar] [PubMed]
- Simons, T. Lead-Calcium Interactions in Cellular Lead Toxicity. Neurotoxicology 1993, fourteen, 77–85. [Google Scholar] [PubMed]
- Centers for Disease Control and Prevention. Blood Lead Levels in Children Aged 1–5 Years-Usa, 1999–2010. MMWR Morb. Mortal. Wkly. Rep. 2013, 62, 245. [Google Scholar]
- Rahal, A.; Kumar, A.; Singh, V.; Yadav, B.; Tiwari, R.; Chakraborty, S.; Dhama, K. Oxidative Stress, Prooxidants, and Antioxidants: The Interplay. BioMed Res. Int. 2014. [Google Scholar] [CrossRef] [PubMed]
- Schulz, E.; Gori, T.; Münzel, T. Oxidative Stress and Endothelial Dysfunction in Hypertension. Hypertens. Res. 2011, 34, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.-C.; Guo, Y.Fifty. Antioxidant Nutrients and Lead Toxicity. Toxicology 2002, 180, 33–44. [Google Scholar] [CrossRef]
- Boghdady, Due east.; Ahmed, N.; Badr, 1000.A. Evaluation of Oxidative Stress Markers and Vascular Hazard Factors in Patients with Diabetic Peripheral Neuropathy. Cell Biochem. Fun. 2012, 30, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-H.; Blomhoff, R.; Jacobs, D.R. Review is Serum Gamma Glutamyltransferase a Marker of Oxidative Stress? Free Radic. Res. 2004, 38, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.-Southward.; Yang, J.H.; Chun, B.Y.; Kam, Due south.; Jacobs, D.R., Jr.; Lee, D.H. Is Serum γ-Glutamyltransferase Inversely Associated with Serum Antioxidants equally a Marking of Oxidative Stress? Gratis Radic. Biol. Med. 2004, 37, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Needleman, H.L.; Gatsonis, C.A. Depression-Level Lead Exposure and the IQ of Children. JAMA 1990, 263, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.; Leviton, A.; Waternaux, C.; Needleman, H.; Rabinowitz, Thou. Longitudinal Analyses of Prenatal and Postnatal Lead Exposure and Early Cognitive Evolution. N. Engl. J. Med. 1987, 316, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Payton, K.; Riggs, G.M.; Spiro, A., 3; Weiss, S.T.; Hu, H. Relations of Bone and Blood Pb to Cerebral Role: The VA Normative Aging Study. Neurotoxicol. Teratol. 1998, 20, 19–27. [Google Scholar] [CrossRef]
- Mahaffey, M.R.; Annest, J.L.; Roberts, J.; Murphy, R.Due south. National Estimates of Blood Pb Levels: U.s., 1976–1980: Association with Selected Demographic and Socioeconomic Factors. N. Engl. J. Med. 1982, 307, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, Y.; Kuh, D. A Life Course Approach to Chronic Illness Epidemiology: Conceptual Models, Empirical Challenges and Interdisciplinary Perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, A.S.; Hu, H.; Hernandez-Avila, Grand. Dietary Calcium Supplementation to Lower Blood Atomic number 82 Levels in Pregnancy and Lactation. J. Nutr. Biochem. 2007, 18, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Rabinowitz, Thousand.; Smith, D. Os Lead as a Biological Marker in Epidemiologic Studies of Chronic Toxicity: Conceptual Paradigms. Environ. Health Perspect. 1998, 106, 1. [Google Scholar] [CrossRef] [PubMed]
- The National Institute for Occupational Safety and Health (NIOSH). Developed Blood Lead Epidemiology & Surveillance (ABLES). 2013. Available online: https://world wide web.cdc.gov/niosh/topics/ables/description.html (accessed on 30 July 2018).
- Sakai, T. Biomarkers of Lead Exposure. Ind. Health 2000, 38, 127–142. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Palazuelos, Due east.; Avila, M.H.; Rios, C.; Muñoz, I.; Jimenez, C.; Cahero, G. Sources of Lead Exposure in Mexico City. Environ. Health Perspect. 1994, 102, 384. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.C.; Stiles, K.One thousand.; Needleman, H.50. Low-Level Lead Exposure, Intelligence and Bookish Accomplishment: A Long-Term Follow-Up Study. Pediatrics 1992, xc, 855–861. [Google Scholar] [PubMed]
- Waller, Thousand.; Osorio, A.M.; Maizlish, North.; Royce, S. Atomic number 82 Exposure in the Construction Industry: Results from the California Occupational Atomic number 82 Registry, 1987 through 1989. Am. J. Public Health 1992, 82, 1669–1671. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-H.; Lim, J.South.; Song, One thousand.; Boo, Y.; Jacobs, D.R., Jr. Graded Associations of Blood Lead and Urinary Cadmium Concentrations with Oxidative-Stress–Related Markers in the US Population: Results from the Third National Health and Diet Examination Survey. Environ. Health Perspect. 2006, 114, 350. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Fiskum, G.; Schubert, D. Generation of Reactive Oxygen Species by the Mitochondrial Electron Transport Concatenation. J. Neurochem. 2002, 80, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Uttara, B.; Singh, A.5.; Zamboni, P.; Mahajan, R.T. Oxidative Stress and Neurodegenerative Diseases: A Review of Upstream and Downstream Antioxidant Therapeutic Options. Curr. Neuropharmacol. 2009, 7, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Obeng-Gyasi, E.; Armijos, R.X.; Weigel, M.1000.; Filippelli, Yard.M.; Sayegh, M.A. Cardiovascular-Related Outcomes in Us Adults Exposed to Lead. Int. J. Environ. Res. Public Health 2018, fifteen, 759. [Google Scholar] [CrossRef] [PubMed]
- Lanphear, B.P.; Rauch, S.; Auinger, P.; Allen, R.W.; Hornung, R.W. Low-Level Lead Exposure and Mortality in US Adults: A Population-Based Accomplice Written report. Lancet Public Health 2018, 3, e177–e184. [Google Scholar] [CrossRef]
- Obeng-Gyasi, E.; Armijos, R.X.; Weigel, M.Thou.; Filippelli, Thou.; Sayegh, Grand.A. Hepatobiliary-Related Outcomes in US Adults Exposed to Atomic number 82. Environments 2018, 5, 46. [Google Scholar] [CrossRef]
- Loghman-Adham, M. Renal Effects of Ecology and Occupational Lead Exposure. Environ. Health Perspect. 1997, 105, 928. [Google Scholar] [CrossRef] [PubMed]
- Cherubini, A.; Ruggiero, C.; Polidori, M.C.; Mecocci, P. Potential Markers of Oxidative Stress in Stroke. Free Radic. Biol. Med. 2005, 39, 841–852. [Google Scholar] [CrossRef] [PubMed]
- Landrigan, P.J.; Todd, A.C. Directly Measurement of Lead in Os a Promising Biomarker. JAMA 1994, 271, 239–240. [Google Scholar] [CrossRef] [PubMed]
Figure 1. Schematic showing how lead exposure acts beyond the life grade of an private.
Figure i. Schematic showing how lead exposure acts across the life course of an individual.
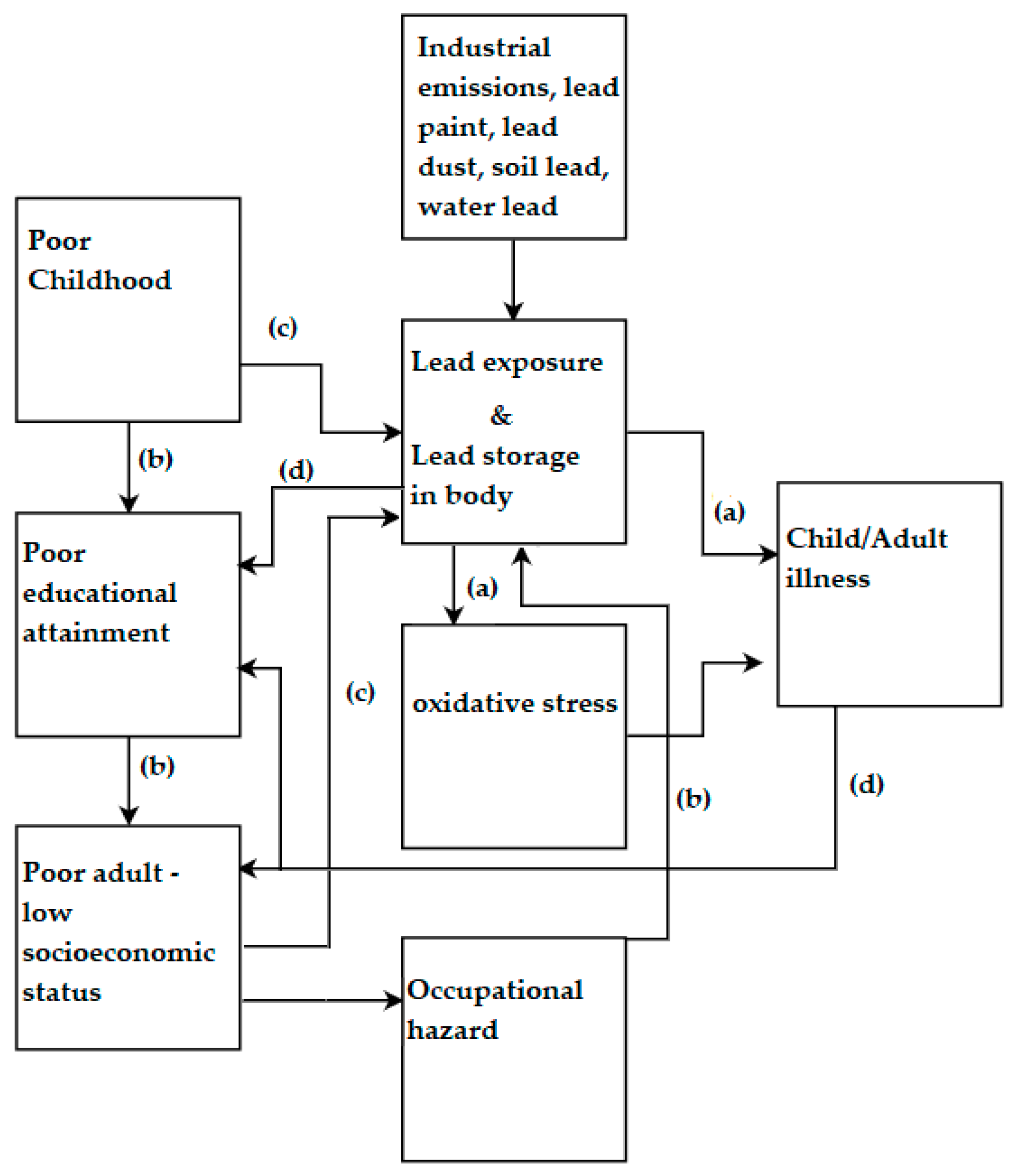
Table 1. Country of Birth and Tertiles of Exposure.
Table one. Country of Birth and Tertiles of Exposure.
| Exposure Level | Born in 50 US States (±SE%) | Born in Mexico (±SE%) | Born in Other Spanish Speaking Country (±SE%) | Born in Other Non-Spanish Speaking Country (±SE%) |
|---|---|---|---|---|
| Northward | 9993 | 621 | 480 | 1054 |
| Tertile 1 | 76.9% (1.one) | 63.seven% (two.ii) + | 79.two% (2.7) | 66.vii% (2.8) |
| Tertile ii | xx.8% (1.0) | 29.nine% (ane.7) ++ | 18.9% (two.seven) | 30.1% (two.four) |
| Tertile 3 | 2.one% (0.2) | 5.ii% (0.9) * | 1.5% (0.3) | 2.6% (0.vi) |
| Total | 100% | 100% | 100% | 100% |
Tabular array 2. Instruction Level and Tertiles of Exposure.
Tabular array two. Education Level and Tertiles of Exposure.
| Exposure Level | Less Than ninth Grade (±SE%) | nine–11th Grade (Includes 12th Grade) (±SE%) | High School Grad/GED Equivalent (±SE%) | Some Higher or AA Degree (±SE%) | Higher Graduate or Above (±SE%) |
|---|---|---|---|---|---|
| North | 802 | 1600 | 2928 | 3587 | 3215 |
| Tertile 1 | 61.one% (2.3) * | 67.4% (ii.2) + | 73.8% (i.2) ^ | 79.1% (1.0) ^^ | 80.3% (ane.4) ^^^ |
| Tertile 2 | 32.1% (ii.0) ** | 28.6% (2.1) ++ | 23.9% (i.2) | eighteen.5% (0.ix) | xviii.4% (i.3) |
| Tertile 3 | v.nine% (0.8) *** | three.1% (0.4) +++ | two.0% (0.iv) | 2.3% (0.4) | 1.1% (0.iii) |
| Full | 100% | 100% | 100% | 100% | 100% |
Tabular array 3. Gender and Tertiles of Exposure.
Table 3. Gender and Tertiles of Exposure.
| Exposure Level | Male (±SE%) | Female person (±SE%) |
|---|---|---|
| Northward | 5858 | 6295 |
| Tertile ane | 67.eight% (1.2) | 82.v% (0.9) * |
| Tertile two | 27.8% (ane.0) ** | 16.6% (0.8) |
| Tertile 3 | iii.vii% (0.3) *** | 0.ix% (0.1) |
| Full | 100% | 100% |
Table 4. Ethnicity and Tertiles of Exposure.
Table iv. Ethnicity and Tertiles of Exposure.
| Exposure Level | Mexican American (±SE%) | Other Hispanic (±SE%) | Non-Hispanic White (±SE%) | Non-Hispanic Black (±SE%) | Other Race-Including Multi-Racial (±SE%) |
|---|---|---|---|---|---|
| Due north | 1032 | 600 | 8342 | 1377 | 802 |
| Tertile 1 | 72.0% (1.9) | 80.vii% (ii.1) * | 76.9% (one.2) ** | 71.v% (1.3) | 66.7% (3.4) |
| Tertile 2 | 23.2% (1.4) *** | 17.3% (ii.4) | 21.1% (1.1) | 24.4% (ane.2) + | 29.vii% (2.ix) **** |
| Tertile 3 | 3.7% (0.7) ++ | 1.six% (0.iii) | 1.8% (0.ii) | 3.seven% (0.5) +++ | ii.9% (0.viii) |
| Total | 100% | 100% | 100% | 100% | 100% |
Tabular array 5. Income and Tertiles of Exposure.
Table 5. Income and Tertiles of Exposure.
| Income | N | Tertile one (±SE%) | Tertile 2 (±SE%) | Tertile 3 (±SE%) |
|---|---|---|---|---|
| $0 to $4999 ^ | 273 | 2.2% (0.3) | 2.viii% (0.5) | iv.0% (i.2) |
| $5000 to $9999 ^ | 399 | iii.2% (0.2) | iv.viii% (0.iv) | five.7% (1.five) |
| $10,000 to $14,999 ^ | 689 | five.5% (0.5) | 7.7% (0.8) | 13.1% (2.four) |
| $15,000 to $xix,999 ^ | 649 | v.2% (0.5) | 7.9% (0.7) | vi.nine% (1.seven) |
| $twenty,000 to $24,999 + | 799 | 7.3% (0.4) | 7.9% (0.vii) | 5.i% (1.5) |
| $25,000 to $34,999 + | 1212 | 10.5% (0.six) | 12.5% (0.8) | 11.six% (1.9) |
| $35,000 to $44,999 + | 1032 | nine.4% (0.6) | 9.six% (0.half dozen) | 10.1% (2.0) |
| $45,000 to $54,999 + | 900 | eight.5% (0.7) | 8.ane% (0.8) | 6.5% (2.2) |
| $55,000 to $64,999 + | 782 | 7.3% (0.4) | 6.9% (0.nine) | 9.2% (two.seven) |
| $65,000 to $74,999 + | 670 | 6.7% (0.5) | 4.half dozen% (0.7) | 5.8% (2.2) |
| $75,000 to $99,999 + | 1306 | 12.eight% (0.viii) | 9.6% (ane.0) | 8.i% (2.3) |
| $100,000 and Over + | 2256 | 21.four% (1.3) | 17.half-dozen% (1.5) | 14.0% (iii.eight) |
| Full | 10,967 | 100% | 100% | 100% |
Table half dozen. Longest Held Occupation and Teritles of Exposure.
Tabular array 6. Longest Held Occupation and Teritles of Exposure.
| Occupation | Tertile 1 (±SE%) | Tertile 2 (±SE%) | Tertile 3 (±SE%) |
|---|---|---|---|
| Adaptation, Food Services | 80.8% (2.7) | 17.7% (2.7) | 1.iv% (0.5) |
| Agriculture, Forestry, Line-fishing | 53.two% (3.5) | 41.8% (3.ix) * | 4.eight% (2.3) ** |
| Construction | 58.2% (three.0) | 35.four% (2.seven) * | 5.1% (1.1) ** |
| Finance, Insurance | 78.0% (three.iv) | 19.9% (3.four) | 1.8% (1.6) |
| Information | 71.7% (4.3) | 27.half dozen% (four.2) | 0.two% (0.2) |
| Manufacturing: Durable Goods | 66.3% (two.3) | 28.vi% (2.i) | 4.4% (0.7) |
| Manufacturing: Non-Durable Goods | 68.half dozen% (2.6) | 28.4% (2.four) | 2.eight% (0.viii) |
| Public Administration | 68.8% (iii.2) | 29.4% (iii.ane) | i.0% (0.6) |
| Existent Estate, Rental, Leasing | 83.0% (5.4) + | 13.8% (four.8) | 2.vii% (1.8) |
| Retail Trade | 79.1% (2.5) | 18.3% (2.2) | 2.0% (0.7) |
Table vii. Age and Clinical Factors and Tertiles of Exposure.
Table 7. Age and Clinical Factors and Tertiles of Exposure.
| Variables | Tertile 1 (±SE) | Tertile 2 (±SE) | Tertile 3 (±SE) |
|---|---|---|---|
| BLL | 1.09 (0.01) | ii.78 (0.02) | 6.40 (0.10) |
| Age * | 44.25 (0.32) | 56.05 (0.54) | 54.77 (1.xiii) |
| GGT ** | 26.54 (0.40) | 33.10 (0.92) | 40.70 (three.77) |
Table 8. Historic period and Clinical Factors and Tertiles of Exposure.
Table 8. Age and Clinical Factors and Tertiles of Exposure.
| Variables | lnBPb Adjusted (95% CI) | p-Value |
|---|---|---|
| GGT + | 0.050 (0.015, 0.085) | 0.007 |
| Age * | 0.827 (0.761, 0.893) | 0.0001 |
© 2018 by the writer. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Eatables Attribution (CC BY) license (http://creativecommons.org/licenses/by/iv.0/).
brunningpissompons.blogspot.com
Source: https://www.mdpi.com/2305-6304/6/3/42/htm